Categories
Abstract
A 48-year-old woman presented with intermittent fever, dyspnea, hand and limb swelling, and purplish plantar spots. Initially diagnosed with pneumonia, she was later found to have mixed connective tissue disease and interstitial lung disease. She required oxygen support, had stable vitals, and exhibited lung crepitations and bilateral pedal edema. Patient had elevated white blood cells, platelets, CRP, creatinine, positive c- Antineutrophil Cytoplasmic Antibody (Anca) and significant proteinuria and hematuria. Initial impression was mixed connective tissue disease with pre renal Acute Kidney Injury (AKI) with differentials of sepsis induced AKI , Anca related Glomerulonephritis (GN) or Infection related GN. Renal biopsy shows a diffuse sclerosing pattern changes with granulomatous nephritis. Negative Immunofluorescence (IF) study concluded sclerosing and granulomatous form of ANCA related pauci-immune glomerulonephritis.
A. 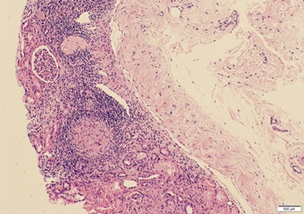 B.
B. 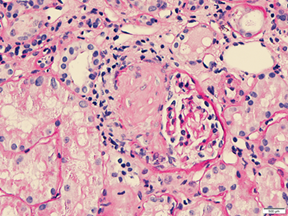
C. 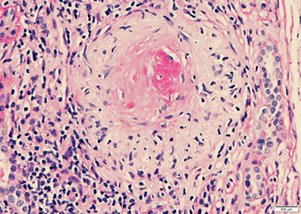 D.
D. 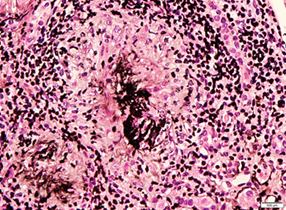
Final diagnosis of Wegener's Granulomatosis@ Granulomatosis Polyangiitis (GPA) was made. Recurrent chest infections with concurrent AKI should indeed raise suspicion for pulmonary-renal syndromes.
References

This work is licensed under a Creative Commons Attribution 4.0 International License.
Copyright (c) 2024 Journal of Clinical and Translational Nephrology